
Have your already heard of Addison’s Disease? Probably not, because it’s one of the rare diseases of our time
What is Addison’s Disease?
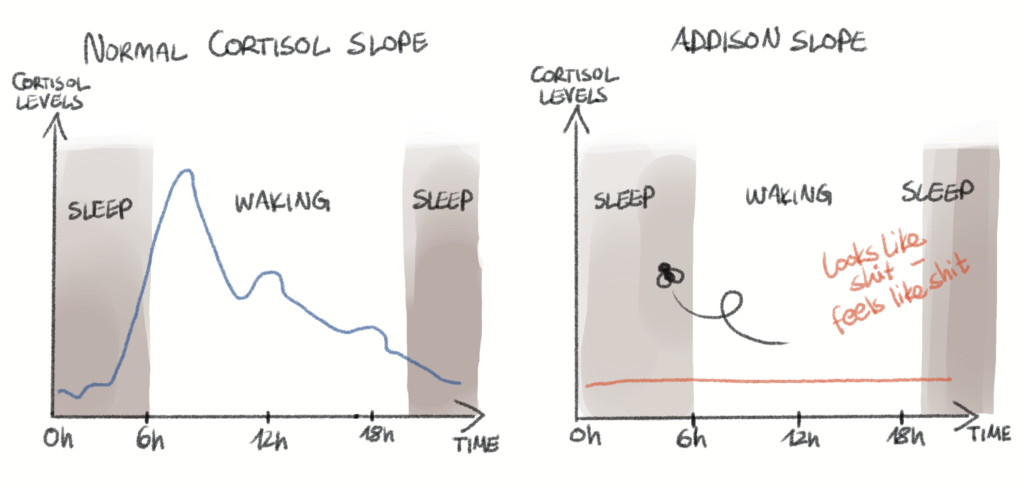
Imagine your body has a built-in stress management system: cortisol, the hormone that kicks in when you’re running from a bear, late to a Zoom meeting, or facing your in-laws. Now imagine that system just… stops working.
That’s Addison’s disease in a nutshell. Officially called primary adrenal insufficiency, it happens when your adrenal glands (those two little guys sitting on top of your kidneys) stop making enough cortisol. Sometimes the problem isn’t the glands themselves but the brain’s messaging system that tells the glands what to do – this is secondary adrenal insufficiency. Either way, the result is the same: not enough cortisol, which your body needs to regulate things like blood pressure, energy, water balance, and your ability to survive Monday mornings.
It’s rare – about 10-40 cases per 100,000 people in Europe. But “rare” doesn’t mean “not a big deal.” Addison’s can seriously mess with daily life.
Why is it problematic? (Spoiler: Because Cortisol Is Kind of a Big Deal)
Without enough cortisol, your body gets confused. You might feel tired, dizzy, nauseous, crave salty snacks (like, really crave them), or even collapse in what’s called an adrenal crisis – which is as scary as it sounds and can be life-threatening.
Fun fact (okay, not that fun): Even when people are diagnosed and treated, adrenal crises still happen in 4 to 10 out of 100 patients each year, and 0.5% of them can be fatal.
The problem isn’t just cortisol being low – it’s that it doesn’t go up when it should. In healthy folks, cortisol ramps up during stress (emotional, physical, or when your toddler smears peanut butter on the walls). But in Addison’s disease, that emergency system is broken.
How is it treated?
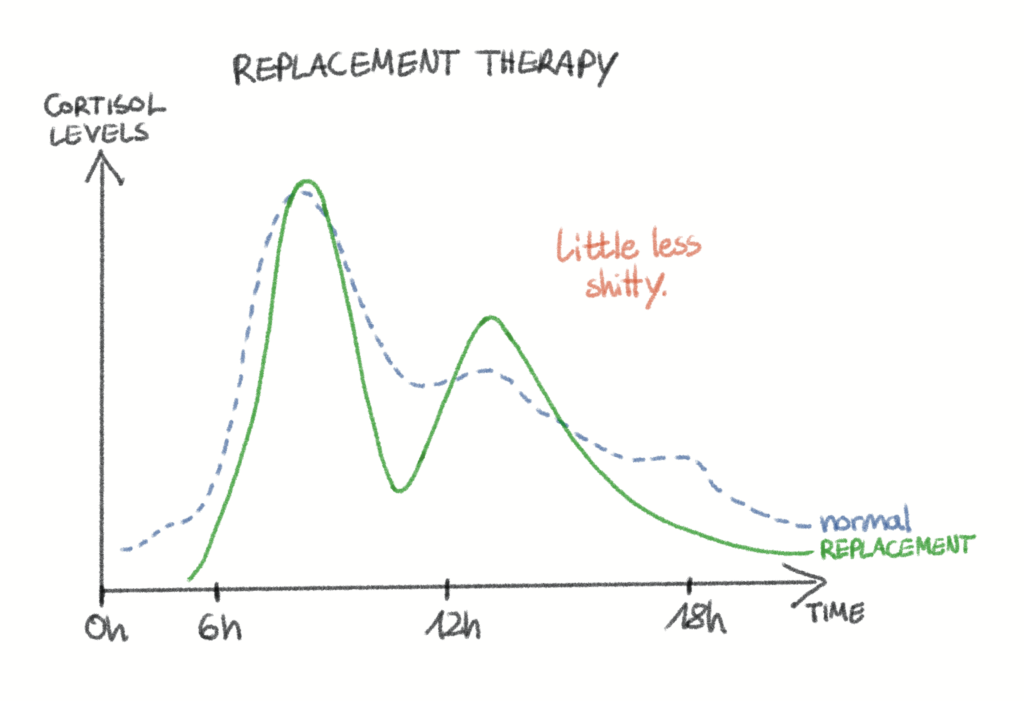
Meet hydrocortisone – Addison’s patients’ daily companion. It’s a synthetic form of cortisol, taken in tablet form to try to mimic the natural daily rhythm of the hormone. Spoiler: it doesn’t do a great job of it.
Patients usually take two to three doses a day, but cortisol in the body normally rises and falls in complex ways throughout the day – and even pulses in ultradian rhythms every couple of hours. A pill can’t keep up with that dance.
And when patients face stress? They have to manually increase their dose. Like, “Hey, I have a flu, I guess I’ll take a bit more hydrocortisone now.” That’s stressful in itself!
Therapeutic education tries to help, teaching patients when and how to increase their dose. But retention is an issue – imagine remembering an emergency plan months after your last workshop. And not everyone responds to the same dose or the same triggers, these huge individual differences make it extra tricky, for both the patients and their physicians.
Why Aren’t There More (or Better) Treatment Options?
Glad you asked. Scientists have been trying to create treatments that better mimic natural cortisol rhythms. Modified-release tablets help a bit. Some countries even have special forms available that get closer to the natural pattern, but many patients are still stuck with the basic pill.
Make space for the cortisol pump. Think insulin pumps for diabetics – but for cortisol. A few small studies, including one called PULSES, have shown promising improvements in energy, mood, and quality of life using an “ultradian” pump (one that mimics the natural pulsatile rhythm). But… clinical trials so far have been small and short-term, so the tech isn’t widely available yet.
There’s also a lack of data on how much cortisol is needed in stressful situations (like exercising or being outside during a heatwave). Without good guidelines, patients either overdose (leading to long-term problems like diabetes or weight gain) or underdose (and risk adrenal crisis). Rock, meet hard place.
What Does This Mean for Daily Life?
Even with treatment, many patients reduce their physical activity, avoid travel, or skip social events because they’re afraid of an adrenal crisis. Some take too much hydrocortisone before workouts, others too little. Neither works out well.
Studies show that up to 40% of people with adrenal insufficiency are frequently on sick leave, struggle to hold down jobs, or face mental health challenges like anxiety and depression. Cortisol isn’t just your stress hormone – it’s your survival hormone.
What’s on the Horizon? (Yes, There’s Hope!)
The good news? Scientists are working hard on solutions:
- Cortisol pumps that deliver the hormone more naturally, mimicking real-life secretion patterns.
- A wearable device (think Fitbit for hormones) called U-RHYTHM that can measure cortisol every 20 minutes – finally letting doctors see real-time data to personalize treatment.
- Clinical trials that aim to show long-term benefits, improve quality of life, and convince health systems that the pump is worth covering.
This dream? A semi-closed loop system for cortisol – just like what’s been achieved for insulin in diabetes.
So, What Should You Take Away from This?
Addison’s isn’t just “low cortisol.” It’s a daily challenge to balance meds, monitor stress, and avoid life-threatening crises. The current treatment helps, but it’s a far cry from perfect.
But between innovative pumps, smarter hormone monitors, and dedicated researchers (and patients!) across Europe, things are finally starting to shift.
So, if you or someone you love is living with Addison’s: you’re not alone, and the future is looking a lot brighter (and hopefully, less stressful).
By the way, May 29th is Addison’s Disease Awareness Day!
References
Barthel A, Benker G, Berens K, Diederich S, Manfras B, Gruber M, Kanczkowski W, Kline G, Kamvissi-Lorenz V, Hahner S, Beuschlein F, Brennand A, Boehm B, Torpy D, Bornstein S. An Update on Addison’s Disease. Exp Clin Endocrinol Diabetes 127(2-03):165-175 (2019). doi: 10.1055/a-0804-2715
Bornstein S, Allolio B, Arlt W, Barthel A, Don-Wauchope A, Hammer G, Husebye E, Merke D, Murad M, Stratakis C, Torpy D. Diagnosis and treatment of primary adrenal insufficiency: An endocrine society clinical practice guideline. J Clin Endocrinol Metab 101(2):364-89 (2016). doi: 10.1210/jc.2015-1710
Burger-Stritt S, Eff A, Quinkler M, Kienitz T, Stamm B, Willenberg H, Meyer G, klein J, Reisch N, Droste M, Hahner S. Standardised patient education in adrenal insufficiency: a prospective multi-centre evaluation. Eur J Endocrinol 183(2):119-127 (2020). doi: 10.1530/EJE-20-0181
Hahner S, Spinnler C, Fassnacht M, Burger-Stritt S, Lang K, Milovanovic D, Beuschlein F, Willenberg H, Quinkler M, Allolio B. High incidence of adrenal crisis in educated patients with chronic adrenal insufficiency: A prospective study. J Clin Endocrinol Metab 100(2):407-16 (2015). doi: 10.1210/jc.2014-3191
Hahner S, Ross R, Arlt W, Bancos I, Burger-Stritt S, Torpy D, Husebye E, Quinkler M. Adrenal Insufficiency. Nat Rev Dis Primers 7(1):19 (2021). doi: 10.1038/s41572-021-00252-7
Nowotny H, Ahmed S, Bensing S, Beun J, Brösamle M, Chifu I, Claahsen van der Grinten H, Falhammar H, Hahner S, Husebye E, Kristensen J, Loli P, Lajic S, Reisch N. Therapy options for adrenal insufficiency and recommendations for the management of adrenal crisis. Endocrine 71(3):586-594 (2021). doi: 10.1007/s12020-021-02649-6
Puar T, Stikkelbroek N, Smans L, Zelissen P, Hermus A. Adrenal Crisis: Still a Deadly Event in the 21st Century. Am J Med 129(3):339.e1-9 (2016). doi: 10.1016/j.amjmed.2015.08.021
Russell G, Kalafatakis K, Durant C 7, Marchant N, Thakrar J, Thirard R, King J, Bowles J, Upton T, Thai NJ, Brooks JCW, Wilson A, Phillips K, Ferguson S, Grabski M, Rogers CA, Lampros T, Wilson S, Harmer C, Munafo M, Lightman SL. Ultradian hydrocortisone replacement alters neuronal processing, emotional ambiguity, affect and fatigue in adrenal insufficiency: The PULSES trial. J Intern Med 295(1):51-67 (2023). doi: 10.1111/joim.13721
Steward PM. Modified-Release Hydrocortisone: Is It Time to Change Clinical Practice? J Endocr Soc 3(6):1150–1153 (2019). doi: 10.1210/js.2019-00046
https://www.addisonsdisease.org.uk/blog/behind-the-research-u-rhythm-2023